What’s the Best Way to Inflate Feline Endotracheal Tube Cuffs?
A prospective study using a feline airway simulator compares four ETT cuff inflation techniques—palpation, minimum occlusive volume, loss-of-resistance, and digital pressure reader—to determine which best achieves optimal intracuff pressures.
What is the most appropriate method for inflating endotracheal tube (ETT) cuffs in feline patients? Which of the 4 described inflation methods is best practice? How does each method impact intra-cuff pressure measurements?
Objective
Compare 4 different ETT cuff inflation techniques using a feline airway simulator (FAS). Assess each technique’s accuracy in creating an appropriate airway seal and minimizing tracheal tissue trauma.
The 4 inflation techniques evaluated were:
- Palpation of Pilot Balloon (P)
- Minimum Occlusive Volume (MOV)
- Digital Pressure Reader Syringe (D)
- Loss of Resistance Syringe (LOR)




Study Design
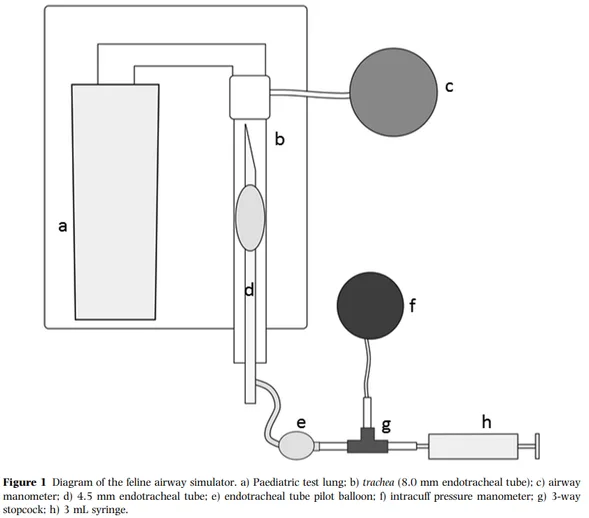
Prospective Design — a Feline Airway Simulator (FAS) was utilized.
Consider: can this model of a cat airway truly replicate all factors that occur in a live cat’s trachea?
The FAS was intubated using a 4.5mm sized, microthin-material & high-volume-low-pressure (HVLP) cuffed ETT to replicate an average sized cat trachea.
Consider: do all adult cat tracheas have the same diameter and a standard ETT size of 4.5mm? How does the material (microthin vs silicone vs PVC) and cuff type (HVLP vs LVHP) impact intracuff pressures?
The 4 ETT cuff inflation techniques (performed in this order):
- Minimum Occlusive Volume (MOV) — ETT cuff was inflated until no audible airway leak was heard during mechanical ventilation. Positive-pressure ventilation (PPV) was provided using a mechanical ventilator set to deliver a peak-inspiratory-pressure (PIP) of 20 cmH₂O.
- Palpation of Pilot Balloon (P) — ETT cuff was inflated based on satisfaction with palpation pressure of the pilot balloon.
- Loss of Resistance Syringe (LOR) — ETT cuff inflated using a 10 mL LOR syringe to temporarily over-inflate until a passive release of pressure occurs.
- Digital Pressure Reader Syringe (D) — ETT cuff inflated to 20–30 cmH₂O using a digital pressure reader syringe.
Consider: how might the accuracy of the MOV technique change when PPV is provided by a ventilator vs manual bag-ventilation? Which is more clinically applicable? Is palpation of an ETT pilot balloon a subjective or objective method? What does “satisfactory palpation pressure” even mean across different individuals? How might the initial over-inflation required for LOR impact the live airway of a cat? Does the digital pressure technique ensure the airway is sealed and protected from pulmonary aspiration & minimizes environmental exposure to inhalant anesthetics?
Each ETT cuff inflation was performed once by members of the anesthesia service — 8 DVMs and 2 Nurses.
Consider: does user experience (anesthesia service vs other sector vs students) impact accuracy of ETT cuff inflation?
ETT cuff inflation for the P + MOV techniques was performed using a brand-new, slip-tip 3mL syringe.
Consider: how does the tip type (slip-tip vs luer-lock) and size of the cuff inflation syringe impact titratability and accuracy of ETT cuff inflation?
All ETT cuffs were deflated to an intracuff pressure of 0 cmH₂O between techniques. After each technique, intracuff pressure was measured using a pressure manometer directly connected to the ETT pilot balloon. Participants were blinded to the pressure manometer’s gauge.

Results
No difference in intracuff pressure was found between techniques overall.
Inflation categories:
- Under-inflation: < 20 cmH₂O
- Optimal inflation: 20–30 cmH₂O
- Over-inflation: > 30 cmH₂O
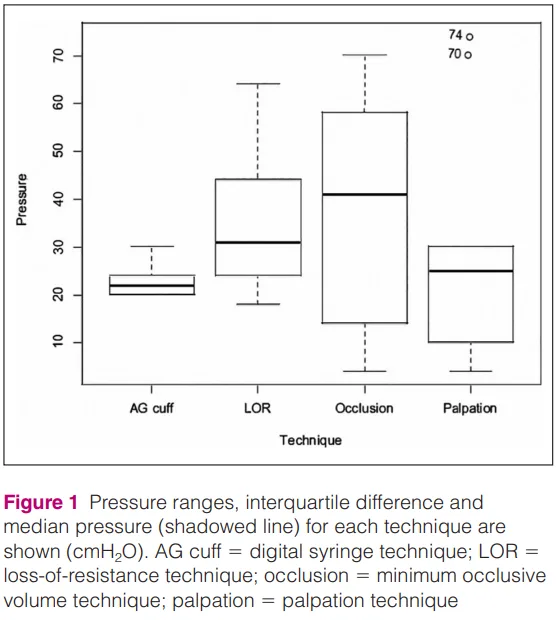
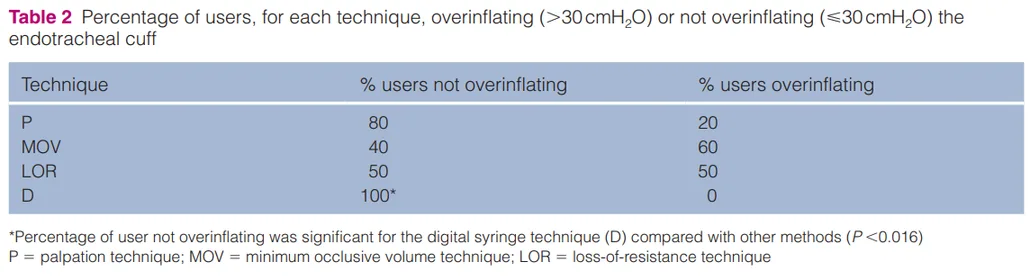
In regard to achieving optimal intracuff values of 20–30 cmH₂O, technique D (digital pressure reader syringe) performed the best compared to the other techniques.
Consider: does this optimal inflation intracuff pressure range (20–30 cmH₂O) guarantee the main goal of a sealed & protected airway is achieved?
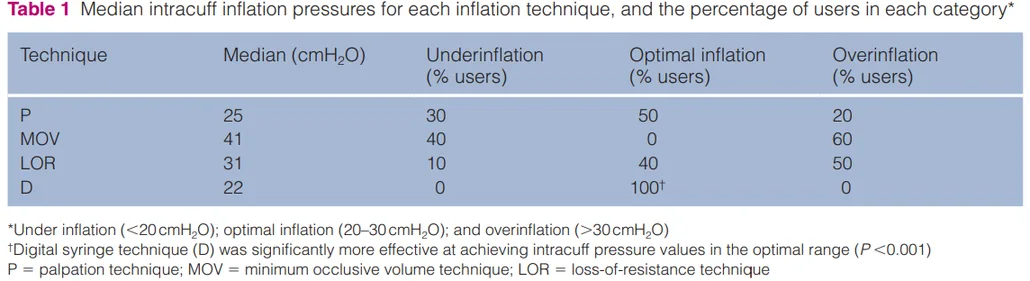
Technique-P had the least amount of over-inflation and Technique-MOV had the greatest amount of over-inflation.
- Technique-P — not over-inflating could also indicate a non-sealed/protected airway & risk of pulmonary aspiration may still be present
- Technique-MOV — using audible cues, rather than objective cues (e.g. achieving an adequate seal of 20 cmH₂O on circuit pressure manometer via leak-testing), may have skewed towards over-inflation
Two techniques had to be repeated due to operator failure in separate participants (1 time for MOV and 1 time for P). The study did not specify the level of experience for those participants that failed initial ETT cuff inflation technique(s).
Conclusions
- The ETT cuff inflation technique of using a digital pressure reader syringe (D) was the most effective at achieving optimal intracuff pressures of 20–30 cmH₂O.
- It is more likely to under-inflate ETT cuffs when utilizing the technique of palpating the pilot balloon (P).
- It is more likely to over-inflate ETT cuffs when utilizing the technique of achieving minimal occlusive volume (MOV).
- There is potential to achieve both under- and over-inflation of ETT cuffs when utilizing the LOR syringe technique.
Limitations
Airway variables not accounted for:
- Properties of live tracheal tissue compared to the FAS model may alter intracuff pressures achieved with each technique
- The goal of optimal intracuff pressures does not evaluate whether a completely sealed and protected airway has been achieved
Equipment variables not accounted for:
- Size of ETT chosen may not be appropriate for all adult cats & may alter properties impacting intracuff pressure
- Material of ETT chosen may have altered properties impacting intracuff pressures and how the material translates and disperses pressure to tracheal tissue
- Utilizing an ETT with a HVLP cuff may have altered properties impacting intracuff pressure compared to ETTs with a LVHP cuff
- Accessibility to some equipment (e.g. digital pressure reader, HVLP cuffed ETT, mechanical ventilator) is not always guaranteed depending on the practice
- Use of a mechanical ventilator versus manual reservoir bag for PPV impacts accuracy of Technique-MOV
Other variables not accounted for:
- User experience with each technique & associated equipment may impact accuracy of technique performance and intracuff pressures achieved
The safest and most effective method of ETT cuff inflation is still undetermined in veterinary patients. While utilizing a digital pressure reader syringe may be most likely to achieve optimal intracuff pressures (20–30 cmH₂O), this method may not guarantee your patient’s airway is protected from the risk of pulmonary aspiration nor minimize the risk of environmental exposure to inhalant anesthetics.
Due to a variety of factors impacting ETT intracuff pressures, it is still recommended to inflate ETT cuffs via leak-testing using the MOV technique with the goal of achieving a circuit pressure of 20 cmH₂O to ensure a sealed & protected airway is achieved.
Get In Touch
Want to learn more?
Whether you're looking for hands-on training or expert consultation, MACvet™ is here to support your team and your patients.