Does Combining Dexmedetomidine with Acepromazine Improve Sedation in Dogs?
A randomized, blinded, crossover study of 6 dogs evaluates whether combining acepromazine or atropine with dexmedetomidine improves sedation quality and how each combination impacts cardiopulmonary parameters.
Does combining dexmedetomidine with acepromazine provide benefits in regard to each of their sedative & cardiopulmonary effects? Does sedation quality improve when both of these sedatives are used in conjunction in canine patients? How are the cardiopulmonary variables impacted when these agents are utilized together in canine patients?
Objective
Determine if the sedation properties of acepromazine & dexmedetomidine are synergistic (i.e. do they potentiate one another’s sedative qualities). Assess how cardiopulmonary parameters change when dexmedetomidine is administered after acepromazine or after atropine.


Study Design
Sample Size = 6 dogs total — very small sample size. Dogs deemed healthy based on labwork (CBC, venous blood gas) and ECG.
Randomized + Blind + Cross-Over Design:
- Randomized = the order of which dogs received each treatment was random & not purposely ordered — prevents results due to chance of when or what order they occurred
- Blind = study observers were unaware of what agent(s) each study dog received — prevents results bias due to observer anticipating a certain result based on previous knowledge of treatment given
- Cross-Over = each dog “crossed-over” or received each treatment protocol with a wash-out period (7 days) in between — prevents results bias due to individual variation
3 Treatment Groups (dexmedetomidine was given 15min after initial drug administration):
- Group 1 = Control — saline + dexmedetomidine 5mcg/kg IV
- Group 2 = Atropine — atropine 0.04mg/kg IV + dexmedetomidine 5mcg/kg IV
- Group 3 = Acepromazine — acepromazine 0.05mg/kg IV + dexmedetomidine 5mcg/kg IV
Parameters assessed by a blinded individual using minimal physical restraint for baseline, 10min post-initial agent, and every 5min for 60min total post-dexmedetomidine: Sedation Scores, ECG + HR, Invasive/Arterial Blood Pressure, Arterial Blood Gas, and Rectal Temp.
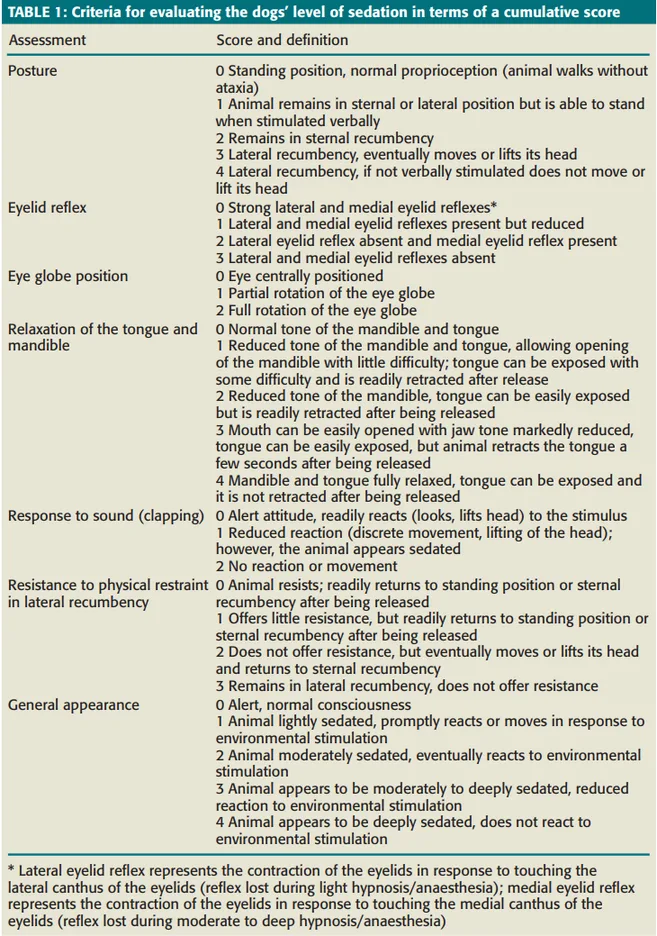
Sedation Scores based on scales utilized in previous studies (Vainio et al 1989 + Kuusela et al 2000) and ranging from scores of 0 to 22. Score 0 = fully conscious. Score 22 = profound hypnosis.
Results
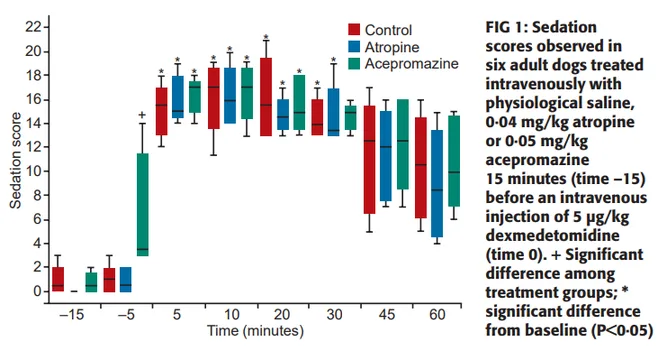
Sedation Effects — NO significant difference in sedation quality between groups.
Sedation 10 minutes post-initial agent:
- Group 1 (saline) = no sedation quality observed
- Group 2 (atropine) = no sedation quality observed
- Group 3 (acepromazine) = light to moderate sedation quality observed — depicted by change in recumbency, but minimal change in responsiveness to external stimuli from baseline
Sedation post-dexmedetomidine administration:
- Compared to Baseline Sedation Scores = significant increase in sedation observed (depicted by: lateral recumbency, mouths and tongues easily opened/retracted manually, reduced to absent response to audible-stimuli, and moderately reduced palpebral reflex)
- Group 1 (saline) + Group 2 (atropine) = increased sedation level for 30min
- Group 3 (acepromazine) = increased sedation level for 20min
- Compared Between Groups Sedation Scores = no significant difference in sedation
Cardiopulmonary Effects — SIGNIFICANT cardiovascular impacts in all treatment groups.
Group 1 (saline) — Effects of dexmedetomidine compared to baseline:
- ECG — significantly increased incidence of dysrhythmias (1st & 2nd Degree AV-Blocks)
- HR — significantly decreased (persisted throughout study period)
- MAP — significantly increased (normalized after 20min post-dexmedetomidine)
Group 2 (atropine) — Effects of dexmedetomidine compared to baseline & control:
- ECG — significantly increased (1st & 2nd Degree AV-Blocks, PVC/VPCs + bigeminy)
- HR — significantly increased; significant tachycardia occurred prior to dexmedetomidine; HR progressively decreased after dexmedetomidine admin, but HRs remained significantly higher than other groups for 45 minutes
- MAP — significantly increased
Group 3 (acepromazine) — Effects of dexmedetomidine compared to baseline & control:
- ECG — significantly increased (all 2nd Degree AV-Blocks); no significant difference in incidence of dysrhythmias prior to dexmedetomidine
- HR — significantly decreased; no significant difference from baseline prior to dexmedetomidine
- MAP — no significant difference overall, but: significantly decreased MAP compared to baseline of acepromazine prior to dexmedetomidine; addition of dexmedetomidine to dogs having received acepromazine did result in a significant, but transient (<10min), increase in MAP; overall MAP in Group 3 was significantly lower than Group 1 within 2 minutes after dexmedetomidine administration
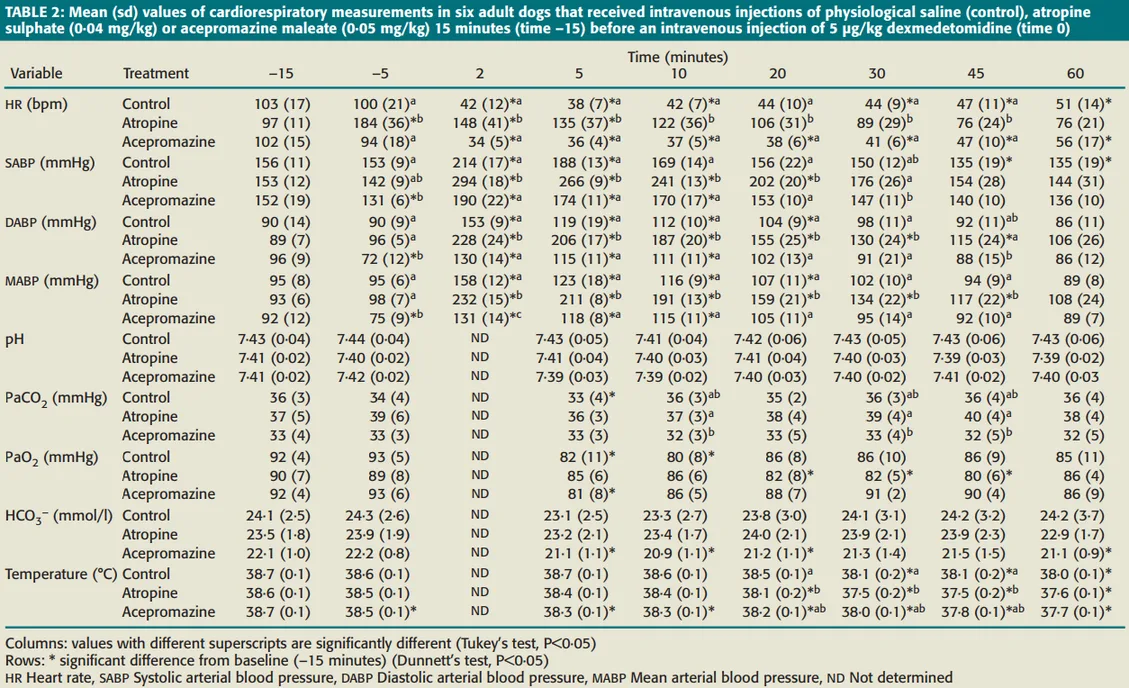
Objective values of additional cardiopulmonary parameters assessed:
Baseline Arterial Blood Gas Parameters compared between groups:
- pH & HCO3 = overall no significant difference
- PaCO2 = significantly decreased (only for Group 3)
- PaO2 = significantly decreased (at different time points)
Baseline Rectal Temperature compared between groups:
- Group 1 (saline) = significantly decreased (only latter duration of procedure)
- Group 2 (atropine) = significantly decreased (only latter duration of procedure)
- Group 3 (acepromazine) = significantly decreased (throughout entire procedure)
Conclusions
The addition of dexmedetomidine to acepromazine showed:
- NO improved sedation quality
- Significantly impacted CV parameters (ECG, HR, and IBP)
- Acepromazine alone showed only significant impact on IBP
- Addition of dexmedetomidine to acepromazine then also significantly impacted HR
- However, dysrhythmias (incidence & severity) were less concerning than when dexmedetomidine was administered after atropine
The addition of dexmedetomidine to atropine showed:
- Severe tachycardia, dysrhythmias, and systemic hypertension
Limitations
Various study factors that may have confounded results:
- Very small sample size (n = 6) — while the cross-over design reduced this concern, the results may not accurately depict the entire canine population
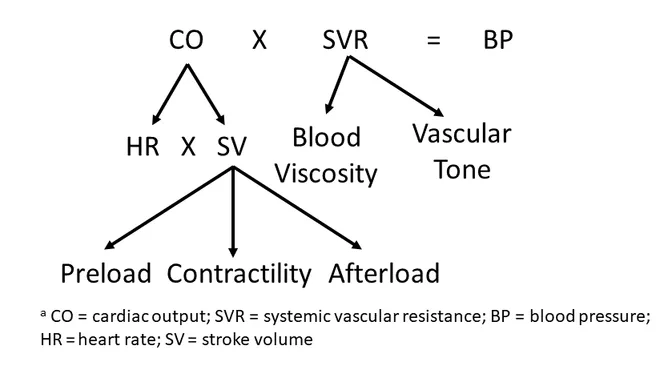
- Direct Cardiac Output was not measured — indirect cardiac output parameters (HR & MAP) may not accurately relay impacts on direct cardiac output monitoring (e.g. thermodilution techniques)
- Impact of adjunct anesthetics not assessed — uncertain if results would have remained the same if injectable or inhalational anesthetics were administered (as in a clinical anesthetic scenario)
- Timing of Drug Admin with Onset of Effects — this study administered dexmedetomidine at the appropriate time point for acepromazine’s onset of effects IV; how these parameters may have changed if acepromazine & dexmedetomidine were administered concurrently at the same time (as might occur in a clinical scenario) is unclear at this time
Combining acepromazine & dexmedetomidine shows no benefits to either sedation quality nor cardiopulmonary parameters. It is contraindicated to give anti-cholinergics prior to dexmedetomidine due to significant negative impacts on cardiovascular parameters.
Want to Learn More?
Whether you're looking for hands-on training or expert consultation, MACvet™ is here to support your team and your patients.